Vibration White Finger
A modelling case study
An epidemiology-based approach to liability ENID modelling has been developed and applied[1]. While based on the same concepts, in practice each scenario-specific ENID model is mathematically unique. This note describes the approach using the example of vibration white finger (VWF[2]). The results agree, within tolerance, with official data.
Brief background
Long term exposure to high intensity vibrations leads to a predisposition to episodes of finger blanching. In severe cases there is loss of dexterity. Cause and severity of VWF are both cumulative in nature. A typical presentation is illustrated below:

The cause of these symptoms is an autonomic[3] constriction of the blood vessels supplying parts of the hands[4]. Episodes of finger blanching may be provoked by vibration, cold weather and wetting with water.
A similar effect is seen in Raynaud’s’ phenomenon (RP) which is of constitutional origin. This initially gave rise to uncertainty as to vibration as a cause.
The first UK compensation settlement was in 1973 (Lambert case) but breach of duty was hotly contested[5]. VWF became a prescribed disease[6] (PD A11) in 1985, exposure management guidance was produced by HSE in 1994 (HS(G) 88) and exposure was quantitatively[7] regulated in 2005.
Summary of model findings and comparison with official data.
The VWF model for the UK suggests there should be 1,430 (plus or minus 520) clear-cut claims every year and 290 (plus or minus 90) weaker ones. The model assumes that everyone with a strong claim will claim before the Limitation period runs out. It is by design an overestimate.
The DWP CRU office keep data on all personal injury liability claims. Under the freedom of information rules they may provide extracts.
The DWP figures for 2015/16 and 17 average out at 1,310 (plus or minus 290).
If this DWP figure is for the number of strong claims then there is a 14% chance that it is different from the number generated by the model.
What we know from this is that the epidemiological method can produce useful liability exposure estimates. The same techniques can be applied to liability ENIDs.
Thus far each liability ENID model is mathematically unique. A bespoke approach to modelling is needed. A set of ENID models would form a useful basis for ENID reserving.
How is it done?
Risk of VWF injury, and liability claim varies with:
- Duration of exposure to vibration (every day for several years)
- Intensity of exposure
- The form of the dose-response relationship
- Age
- Severity (and the important distinction from constitutional RP)
- Probability of proof of breach
- Probability of EL cover (varies with self-employment rates)
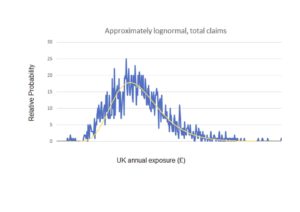
The preference is to find a single well conducted study which provides a valid diagnostic dose-response function based on proven metrics and at the same time shows how severity varies with dose. Several such studies, if homogeneous in design, could be pooled but in practice there is only one study[8] for the UK which simultaneously passes these tests.
Exposures have been measured for a wide variety of trades and follow a log-normal distribution. Model users are permitted to vary the log-normal distribution to suit their own insurance portfolio. Duration of exposure comes from knowledge of the occupational tenure in those trades.
So, for a given intensity and duration of exposure, the odds ratio can be calculated. From this, an estimate of the excess risk is derived and knowing the number of men with that level and duration of exposure leads to the expected number of VWF cases per year. The odds ratio also determines the severity profile. Slight injuries should be more difficult to distinguish from constitutional Raynaud’s disease and so will be less likely to lead to claims. The model user can vary the probability for claims for slight injury. Being higher risk, a higher proportion of damages would be expected as claimant legal fees in slight injury claims. The model user can vary this proportion according to their experience of claims.
Exposure intensity also provides a measure of the probability of proof of breach, though for severe VWF cases the proof of breach is strongly implied in the injury itself.
Age-dependent scales for general damages and for Smith and Manchester damages (for higher severity cases only) were generated from data developed from official statistics. There is no meaningful medical intervention.
Number of claims at a given severity x severity (£) = liability exposure (£). Simply add together the values at each level of injury severity.
By weighted random sampling across all the available variable space a loss probability distribution curve (histogram) is generated.
Given that the vibration exposure data was taken directly from identified trades, the liability exposure is given as an output from the model for each trade and from this insurers can assess their own exposure according to market share. Construction has the greater share of VWF liability.
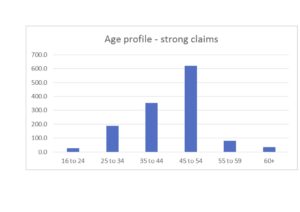
For those who want to understand the characteristics of the injured population a typical age profile is provided:
This VWF model, and several liability ENID models based on the same techniques are available for sale to liability insurers and to those with a specialist interest, such as manufacturers and employers.
andrew@reliabilityoxford.co.uk
[1] Although each ENID model is unique, the same principles have been applied to:
- night shift work as a cause of breast cancer,
- e-cigarettes as a cause of asthma,
- an occupational cause of heart disease,
- an occupational cause of stroke,
- processed meat as a cause of two kinds of cancer
- the effect of antimicrobial resistance on some cancer claims
These ENID models are available for sale to liability insurers and those with a specialist interest e.g. manufacturers.
[2] Over time, the scope of injuries caused by exposure to excessive vibration has been expanded and the term VWF has been replaced by Hand Arm Vibration Syndrome (HAVS). HAVS includes VWF. The model was for VWF, not HAVS.
[3] Autonomic means; in the form of a reflex response. Like all reflexes the trigger and degree of response can be varied by experience – a training effect.
[4] As a distraction, experts were temporarily wedded to the idea that skin calluses were the cause, this was a theory promulgated by IIAC in the 1970s.
[5] In Joseph v MOD (1980) the MOD successfully defended on breach of duty.
[6] The BMA Occupational Health Committee had recommended prescription in 1967.
[7] According to HASAW regulation (1974) risks should be reduced “as far as is reasonably practicable”. This was better defined for vibration in 2005: The Control of Vibration at Work Regulations 2005 (the Vibration Regulations), came into force on 6 July 2005. Specific health surveillance measures were included in this regulation. Around 4% of working men were exposed at above the 5ms-2 (8 hour average) duty level. Around 255,000 men at work already had clearly diagnosable VWF.
[8] The best study for modelling purposes is Occup Environ Med (2003) Vol.60 p 16–26. M J Griffin, M Bovenzi, C M Nelson. Dose-response patterns for vibration-induced white finger.